Takeaways from the past PNS annual meeting
The 2026 Annual Meeting of the Peripheral Nerve Society (PNS) took place in Maastricht from 13 to 16 June 2026 and brought together clinicians, researchers, industry partners and patient advocacy organisations working on peripheral neuropathies. For the CMT community, the meeting showed a field that is moving quickly: not through one single “breakthrough”, but through many connected advances in genetics, disease models, treatment development, rehabilitation, outcome measures and patient partnership. The scientific programme included a large Charcot-Marie-Tooth and Related Neuropathies Consortium section, with posters and oral presentations dedicated to CMT, hereditary transthyretin amyloidosis, and other inherited neuropathies.
This article focuses on Charcot-Marie-Tooth and related inherited peripheral neuropathies. It does not cover acquired neuropathies such as diabetic, inflammatory, toxic or traumatic neuropathies, except where they were discussed as conditions that can be confused with inherited disease.

1. Genetics and diagnosis: naming the disease remains the first step
A strong message from Maastricht was that genetic diagnosis is no longer only about giving a condition a name. It is becoming a key that can open the door to better care, family counselling, research participation, and future subtype-specific trials.
Several studies showed how diverse CMT is across countries and populations. Cohorts from Saudi Arabia, India, Japan, Ghana, Brazil and Europe confirmed that the most frequent genes can differ by region. In some areas, recessive forms are more common because of family structure and consanguinity. In others, the usual genes such as PMP22, MPZ, MFN2 and GJB1 remain frequent, but many rare genes also appear. The practical message for patients is clear: “CMT” is not one disease. It is a large family of inherited neuropathies, and the exact genetic subtype increasingly matters.
Researchers also described newly recognised or expanded genetic causes of inherited neuropathy, including variants in genes such as NARS1, TUBB3, VRK1, GBF1, MPV17, ITPR3, ATP1A1, MME, VWA1, HINT1, DNAJB2 and others. Some of these genes can cause “pure” CMT-like neuropathy, while others can involve the brain, spinal cord, muscles, eyes or autonomic system. This helps explain why some people with inherited neuropathy have symptoms that do not fit the classic CMT picture.
New diagnostic technologies were another major topic. Long-read sequencing, RNA sequencing, pangenome analysis and artificial intelligence were presented as tools that may help solve cases that remain genetically unexplained after standard testing. These methods can detect changes that older tests may miss, including hidden structural changes, deep intronic variants and repeat expansions such as those seen in RFC1/CANVAS. A machine-learning tool, PredictNeuropathy, was also presented to help distinguish hereditary demyelinating neuropathies from acquired inflammatory neuropathies, a distinction that can be difficult in real clinical practice.
For patients, this means that an “unsolved” genetic result today may not remain unsolved forever. As testing improves, it may be worth discussing with a specialist whether older genetic results should be revisited, especially for people with a strong family history, childhood onset, foot deformities, long-standing unexplained neuropathy, or symptoms affecting several family members.
2. Understanding disease mechanisms: better models, better targets
Many presentations focused on understanding what is impaired inside nerve cells and Schwann cells. Schwann cells are the support cells that wrap peripheral nerves in myelin, the insulating layer that helps nerve signals travel efficiently. Axons are the long nerve fibres that carry signals to muscles and sensory organs. Some forms of CMT mainly affect myelin; others mainly damage axons; many involve both.
Researchers are now using patient-derived stem cells, motor neurons, sensory neurons, Schwann cell models, organoids and “assembloids” to study CMT in human-like systems. These models are important because animal models do not always fully reproduce human disease. Several groups presented work using induced pluripotent stem cells, which are stem cells made from a patient’s own cells and then turned into nerve or muscle-related cells in the laboratory.
These models are being used to study CMT1A, CMT1B, CMT2D, CMT4C, HSAN1 and other inherited neuropathies. They allow researchers to watch disease processes in the lab, test possible treatments earlier and compare different genetic subtypes. Some studies looked at myelin formation, others at axonal transport, mitochondria, stress responses inside cells, DNA repair, protein production and nerve-muscle communication.
One clear theme was that CMT is not simply “weak nerves”. In different subtypes, the problem may involve too much of a protein, too little of a protein, a toxic version of a protein, poor energy production, impaired transport along axons, faulty myelin maintenance, or abnormal stress signals inside cells. This is why future treatments will probably need to be matched to disease mechanism and genetic subtype.
3. Gene therapy for CMT is becoming more concrete
A dedicated lecture by Prof. Kleopas Kleopa reviewed the current status of gene therapy development for CMT neuropathies. The lecture made clear that gene therapy is no longer just a distant concept, but a growing set of strategies. These include replacing a missing gene, lowering an overproduced gene, silencing a harmful copy of a gene, editing DNA, or compensating for a damaged pathway.
The lecture also explained the main challenge: delivery. For axonal forms such as CMT2, the target may be motor neurons, sensory neurons or long axons. For demyelinating forms such as CMT1 and CMT4, the target may be Schwann cells. Researchers are testing viral carriers such as AAV, as well as non-viral approaches such as nanoparticles. Delivery routes include intrathecal injection, intravenous injection, intramuscular injection and, in some experimental work, injection around or into nerves.
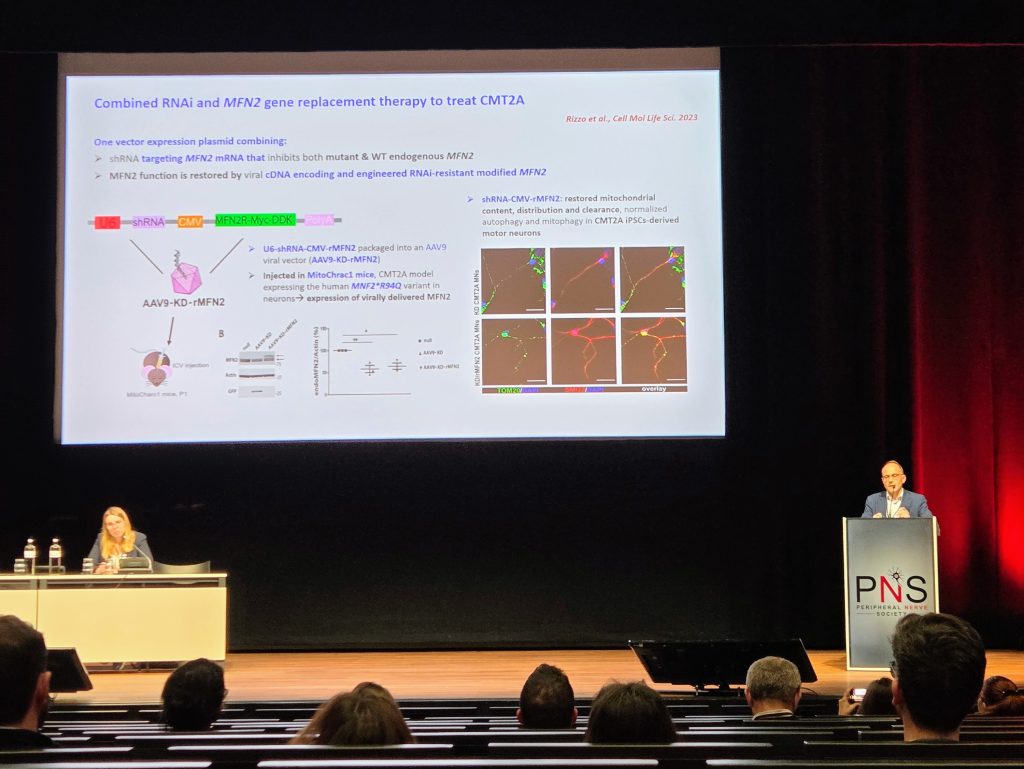
Several CMT subtypes were highlighted. In CMT1A, where the problem is usually too much PMP22, different groups are trying to safely reduce PMP22 levels using siRNA, microRNA, shRNA, antisense approaches, nanoparticles or AAV-based tools. In CMT1X, caused by GJB1/Cx32 mutations, gene replacement aims to restore the missing connexin function in Schwann cells. In CMT2A, caused by MFN2 mutations, researchers are exploring ways to restore mitochondrial balance by replacing, increasing or correcting mitofusin function. In CMT2D, linked to GARS1, approaches include tRNA-based gene therapy and other ways of calming the cell stress response. In rarer forms such as CMT4J, CMT4C, CMT4A, CMT4D, CMT2S/SMARD1 and CMT2E, gene replacement, gene silencing or gene editing strategies are being explored.
The patient message is one of cautious optimism. Most gene therapy projects are still in laboratory or animal stages, and only some are approaching or entering human testing. However, the direction is important: the field is moving away from “one treatment for all CMT” and toward treatments designed for specific genetic causes.
4. Treatment research: from disease-specific drugs to muscle activation
Treatment research at Maastricht covered several different approaches. Some aim to correct the root cause of a subtype. Others aim to improve nerve function, muscle activation, myelin repair, or cellular stress responses.
In CMT1A, several studies focused on reducing PMP22 or improving Schwann cell function. In CMT1B and CMT1E, researchers explored stress pathways inside myelin-producing cells and possible ways to improve protein handling. In GDAP1-related CMT and CMT2J, HDAC6 inhibition was presented as a possible strategy to improve axonal transport and nerve function in models. In CMT2D, researchers presented both gene-based and drug-based approaches aimed at reducing the harmful stress response caused by GARS1-related disease. In SORD-related CMT, urine and blood biomarkers such as sorbitol and xylitol were discussed as tools that may support diagnosis and future trials.
A small clinical study of repeated allogeneic mesenchymal stromal cells in CMT1A from ENCell reported that the treatment was safe and well tolerated in a small number of adults, with exploratory signals that need confirmation in larger studies. Other work looked at focused ultrasound to help gene therapy reach peripheral nerves more efficiently, and improved AAV targeting of Schwann cells to lower future gene therapy dose and improve safety.
The SYNAPSE-CMT Ignaseclant trial
A late-breaking oral presentation, also described in a press release from NMD Pharma, presented Phase 2a data from the SYNAPSE-CMT study of ignaseclant, formerly NMD670. This is not a gene therapy. It is an oral investigational medicine designed to improve skeletal muscle activation by targeting the ClC-1 chloride channel. The trial enrolled 81 ambulatory adults with genetically confirmed CMT1 or CMT2, used a randomized, double-blind, placebo-controlled design, and tested twice-daily ignaseclant for 21 days with follow-up to day 28.
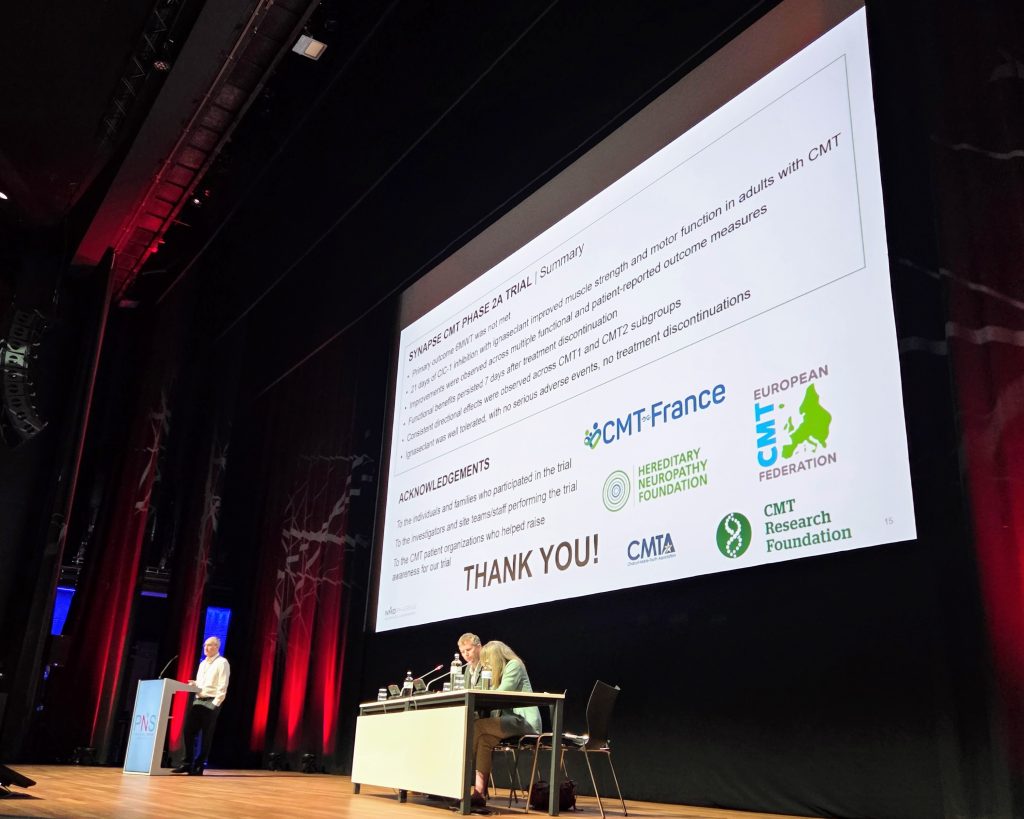
The primary endpoint, the six-minute walk test, did not show a treatment effect in the abstract. However, the company reported encouraging signals in secondary measures, including the CMT Functional Outcome Measure, hand grip strength, the 9-hole peg test and trends in lower-limb outcomes. Reported adverse events were mild or moderate, with no serious adverse events or study discontinuations. These results are early and need larger and longer trials, but they are important because the treatment approach may be relevant across several CMT subtypes, rather than one genetic subtype only.
5. Trial readiness: measuring CMT better
Another major theme was trial readiness. A treatment can only be tested properly if researchers can measure whether it helps. For CMT, this is difficult because progression is often slow, symptoms vary between subtypes, and the daily impact of disease is not always captured by traditional clinical tests.
Several studies therefore focused on clinical outcome measures. These included the CMT Pediatric Scale, the CMT Functional Outcome Measure, the CMT Neuropathy Score, the CMT Infant Scale, and virtual or remote versions of some assessments. One large pediatric natural history study showed that children with CMT do progress measurably over one year, but that the rate of progression differs by age and genetic subtype. This type of information is essential for designing clinical trials.
Training and certification of clinical evaluators was another key topic. If the same test is performed differently at different hospitals, trial results become less reliable. The CERTIFYCMT work focused on how to train evaluators so that strength, balance, dexterity and functional tests are performed consistently. Other projects are translating and diversifying training resources so that trial readiness is not limited to a few countries or centres.
Digital outcome measures are also advancing. Wearable sensors were presented as a feasible way to measure real-world gait and balance in adults with CMT1A. The DANCER project presented smartphone video-based movement analysis as a possible future tool for collecting detailed gait information at scale, outside highly specialised laboratories. These approaches could make future trials more inclusive and more realistic, because they measure how people move in daily life, not only during a clinic visit.
6. Biomarkers: looking for measurable signs of disease activity
Researchers also presented work on biomarkers. A biomarker is a measurable sign that can help diagnose a disease, follow progression, or understand whether a treatment is having an effect.
In CMT and related inherited neuropathies, proposed biomarkers included blood neurofilament light chain, plasma proteins, RNA markers, urine and serum polyols in SORD-CMT, nerve ultrasound, muscle MRI, MR neurography, skin biopsy and small fibre tests. For hereditary transthyretin amyloidosis, several studies examined biomarkers of nerve damage, autonomic involvement, eye involvement and response to therapy. For CMT, the field is still searching for biomarkers that are sensitive enough, subtype-specific enough and practical enough for clinical trials.
The most important point for patients is that biomarkers may one day help researchers detect whether a treatment is working before major clinical changes are visible. This could shorten trials and reduce uncertainty, especially in slowly progressive forms of CMT.
7. Rehabilitation, orthotics and daily function: research that matters now
Not all important research is about future drugs. Several Maastricht presentations focused on walking, balance, fatigue, orthotics, foot mechanics, sleep, physical activity and quality of life. These topics are central to daily life with CMT.
Studies on foot structure and walking showed that cavus or cavovarus feet can change how forces pass through the foot, often increasing pressure on the outside of the foot. This may help explain pain, instability and injury risk in some people with CMT. Other work found that the Timed Up and Go test may help identify people at greater fall risk.
In children and adolescents, personalised insoles were associated with improved walking speed and stride length, and with fewer reports of ankle instability, falls and trips after use. Orthotic adherence and satisfaction were also studied, highlighting the importance of follow-up, adjustment and practical support.
Balance rehabilitation was another strong theme. Researchers presented co-designed balance programmes, home-based rehabilitation, stabilometric platforms and neuromuscular electrical stimulation. Co-design means that people living with CMT help shape the intervention, rather than researchers designing it alone. Participants emphasised that balance programmes should be flexible, safe, adapted to different ability levels and realistic for people whose symptoms vary from day to day.
Fatigue and sleep were also discussed. Studies in children showed that fatigue is common and multidimensional, affecting endurance, behaviour, recovery after activity and family life. Sleep disorders, including obstructive sleep apnoea and periodic limb movement disorder, were reported in a significant proportion of children in one study. This reinforces that CMT care should not focus only on feet and hands. Fatigue, sleep, pain, mental health, school, work, and social participation also need attention.
Most meaningful research for patients’ daily lives
Among the many studies presented, the research with the most immediate impact for patients was the work focused on walking, falls, fatigue, sleep, physical activity and practical rehabilitation. These are the issues that often decide whether a person with CMT can go to school, work, travel, exercise, socialise or remain independent. One study in children and adolescents found that personalised insoles were linked to better walking speed and stride length, and reports of ankle instability, falls and trips dropped after insole use. Another study showed that a simple clinic test, the Timed Up and Go, may help identify people with CMT at higher risk of serious falls, which could allow earlier physiotherapy, orthotic review and home-safety planning. Balance rehabilitation studies also suggested that objective balance platforms may help measure whether rehabilitation is really improving stability.
Fatigue and sleep research was equally important: in one paediatric study, fatigue was reported by 80% of children, and sleep disorders were found in 61% of those who completed sleep testing, including obstructive sleep apnoea and periodic limb movement disorder. The authors concluded that fatigue and sleep problems should be actively screened in routine CMT care, especially in children with more severe disability. The co-designed physical activity work also stood out because it started from the realities of families: exercise programmes need to be fun, flexible, adapted to fatigue and pain, supported by professionals, and easier to access through remote options when needed. Looking slightly further ahead, the ignaseclant SYNAPSE-CMT study was also meaningful for patients because it tested an oral treatment approach aimed at improving muscle activation across genetically confirmed CMT1 and CMT2, with reported signals in hand grip strength, dexterity and lower-limb functional measures; it remains investigational and will need larger, longer studies.
Taken together, these studies remind us that “high-impact” CMT research is not only about future cures. It is also about reducing falls, improving walking confidence, managing fatigue, recognising sleep problems, and helping people with CMT participate more fully in everyday life.

8. Related inherited neuropathies: lessons beyond classic CMT
The meeting also included related inherited neuropathies such as hereditary transthyretin amyloidosis, CANVAS/RFC1 disease, HSAN1, SORD neuropathy, MNGIE, Friedreich’s ataxia with neuropathy, hereditary motor neuropathies and mitochondrial or metabolic disorders that can mimic CMT.
These studies matter to the CMT community because they show common challenges: delayed diagnosis, misdiagnosis, the need for better biomarkers, and the importance of matching patients to the right treatment or trial. Some inherited metabolic or amyloid neuropathies now have disease-modifying treatments, making early diagnosis especially important. The lesson is that careful diagnosis is not academic; it can change care.
9. The patient coffee chat panel
A particularly important moment was the Patient Advocacy Group Partners: Patient Panel Coffee Chat, scheduled as an open meeting during the PNS programme on Sunday 14 June. Four people living with peripheral neuropathy brought patient voices directly into a scientific meeting mainly attended by researchers and clinicians. We are grateful to the PNS team for including this panel into their meeting program.

This type of session matters because research can easily focus on what is easy to measure, rather than what matters most in daily life. Patients can explain the real burden of delayed diagnosis, fatigue, pain, falls, braces, access to physiotherapy, uncertainty, family planning, work, school and the emotional impact of progressive disease. Their contribution helps researchers design better studies, choose more meaningful outcome measures and communicate results in ways that patients can understand and use.
For ECMTF, the coffee chat panel reflected a central principle: patients should not be consulted only after research decisions are made. They should help shape priorities from the beginning.
10. The ECMTF poster and the Antwerp-to-ECRA pathway
ECMTF also presented a poster on “Advancing clinical trial readiness in Charcot-Marie-Tooth disease”, summarising scientific and strategic outcomes from the 2nd European CMT Specialists Conference held in Antwerp in October 2025. The poster described Antwerp as more than a conference: it was framed as an implementation platform to align clinical care, outcome measures, data sharing, therapeutic development and patient partnership in CMT.
The poster reported more than 130 participants, 21 selected oral presentations, 32 scientific posters, 4 webinars, 6 backstage expert interviews and 6 Daniel Tanesse awards. More importantly, it listed concrete deliverables: medical training recommendations, a data-sharing framework aligned with GDPR and the European Health Data Space, an AI-in-CMT report, a model multistakeholder research project, rehabilitation guidance, outcome measure standardisation, a digital care strategy and a cooperative R&D framework built around “patients as partners.”
The poster also highlighted the European CMT Research Association (ECRA) as an implementation engine for the next phase. ECRA is intended to connect scientists, clinicians, allied health professionals, patient advocates and industry partners, with the aim of building trial-ready cohorts, mentoring young researchers, coordinating webinars and workshops, and supporting joint grant applications.
During the opening CMTR session, the 3rd CMT Specialists Conference was announced; it will take place in Cyprus at the CING on 21-23/10/2027.
11. New partnerships: moving from lab bench to bedside
A recurring message from Maastricht was that CMT research cannot move forward through isolated projects alone. New therapies require a full ecosystem: patients with confirmed diagnoses, registries, trained clinical evaluators, agreed outcome measures, biomarkers, trial-ready centres, ethical data sharing, industry collaboration and patient organisations that keep research focused on real-life priorities.
The ECMTF poster captured this shift with a simple working principle: patients as partners, data as infrastructure, outcomes as regulatory currency, and ECRA as implementation engine. It also highlighted partnership models such as the CureCMT Doctoral Training Network, involving leading scientists across several countries, patient organisations and industry partners, and the European Patient Journey in CMT, aimed at earlier diagnosis and better care pathways.
This is what “from lab bench to bedside” means in practice. A discovery in a cell or mouse model is only the first step. To become a treatment, it must pass through safety testing, clinical trial design, patient recruitment, outcome measurement, regulatory review, reimbursement discussions and real-world access. Patient organisations such as ECMTF can help connect these steps and make sure that future therapies are developed with patients, not only for patients.
12. What patients can take from Maastricht
The Maastricht meeting showed a field with strong momentum. For patients and families, the key messages are practical.
- First, genetic diagnosis is increasingly important. It can affect prognosis, family counselling, eligibility for studies and future access to subtype-specific therapies.
- Second, treatment development is active across many CMT subtypes. Some approaches are still early, but the number and diversity of projects is increasing.
- Third, rehabilitation, orthotics, balance training, fatigue management, sleep assessment and psychosocial care remain essential now. They are not secondary to “real” research; they are part of improving life with CMT.
- Fourth, clinical trials will depend on better measurement. Outcome scales, digital tools, biomarkers and patient-reported data are becoming part of the treatment pipeline.
- Finally, patient partnership is becoming central. The coffee chat panel, ECMTF’s poster and the growth of ECRA all point in the same direction: CMT research will move faster and better when patients, clinicians, researchers, industry and policy actors work together.